Patients who undergo lung volume reduction surgery (LVRS) for advanced emphysema may survive longer with fewer complications than they did in the past. What’s more, they may do better than patients who undergo endobronchial valve (EBV) placement. J.W. Awori Hayanga, MD, MPH
J.W. Awori Hayanga, MD, MPH
That’s according to new risk-adjusted findings presented at the 2025 Society of Thoracic Surgeons Annual Meeting in January. The STS said in a news release that despite shorter hospital stays, lower charges and lower Elixhauser Comorbidity Index (ECI) scores — which quantify pre-existing conditions and how they affect treatment outcomes — investigators found that patients who underwent EBV placement ultimately had more complications and higher longitudinal risk of death than those who received LVRS.

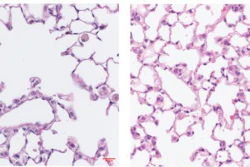
“The standard treatment using bronchodilators is typically sufficient for most patients, but often the disease is very severe and has no therapeutic options,” said lead study author J.W. Awori Hayanga, MD, MPH, professor of thoracic surgery at West Virginia University Medicine in Morgantown.
“Lung transplantation is not always a durable solution because of the shortage of donors compared to the demand for organs,” Dr. Hayanga said. “The potential of surgical volume reduction was duly explored in the late 1990s in patients with severe emphysema. The surgical approach, however, did not gain broad popularity because of the high mortality of 8% and the small group of patients believed to benefit from the procedure.”
EBVs gained popularity following trials in the 2010s and FDA approval in 2018. Despite this, Dr. Hayanga said that long-term data on how patients with severe emphysema fared after EBV placement is limited. His research team examined mortality and procedure-related complications in patients with advanced emphysema using doubly robust, risk-adjusted models that compared patient outcomes after EBV placement versus LVRS.

“We observed that patients undergoing EBV placement have higher occurrences of various complications over time, often need a greater number of interventions and even suffer higher mortality compared to those undergoing LVRS in contemporary surgical practice, where techniques have become much less invasive than they were 20 years ago when (these) surgical options were first evaluated,” Dr. Hayanga said.
The team examined data from the Centers for Medicare and Medicaid Services (CMS) inpatient claims database, evaluating 3,219 patients with severe emphysema undergoing either LVRS or EBV between Jan. 1, 2019, and Dec. 31, 2022. Of those included in the study, 2,378 received LVRS and 841 received EBV placement.
Prior to risk adjustment, EBV recipients had lower ECI scores, shorter hospital stays and lower hospital charges compared to those who underwent LVRS. Most LVRS procedures (1,897) were minimally invasive, video-assisted thoracoscopic or robotic surgeries, while 481 were open surgeries.

“Medicare beneficiaries who undergo EBV present with fewer comorbidities, but after risk adjustment they have higher mortality and procedure-related morbidity than those undergoing LVRS,” Dr. Hayanga said.
The team said that these results suggest the need to revisit multidisciplinary decision-making about the role of surgery over bronchoscopic interventional therapy in the management of advanced emphysema.
“Outcomes after surgery were better than previously reported and were often better than those after valve placement,” Dr. Hayanga said. “It is likely that patients do far better after surgery than they used to.”